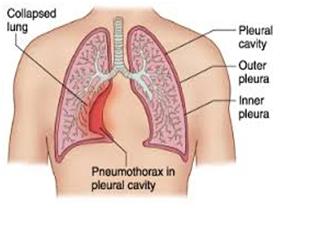
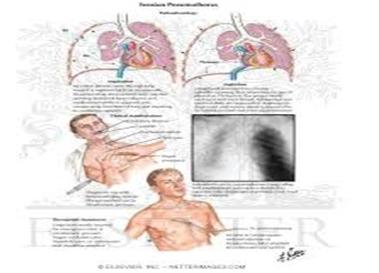
DEFINITION:-
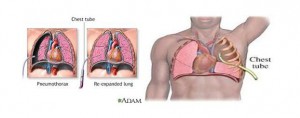
It is a collection of air in the pleural space normally the pressure in the pleural space is negetive compare to atmospheric presure. This negetive pressure is require to maintain lung inflation.
ETIOLOGY:-
It may be due to internal or external trauma which can be differentiate according to the type of trauma & site of involve it.
TYPES:-
1. Closed pneumothorax:-
There is no association with external injury or wound this is most common form of sponteneous pneumothorax.
Cause:-
A. Injury to the lungs due tio any mechanical ventilation
B. Injury to the lungs due to any broken ribs
C. Rupture of the bells & belbs
D. Perforation
E. Under weight smokers
2. Open pneumothorax:-
In this type of pneumothorax air enter into pleural space due to external injury or trauma. for eg:- stab wound , gun shoot , any surgical procedure of thorax
3. Tension pneumothorax:-
Pneumothorax with rapid accumulation of air into pleural space causinghigh intrapleural pressure with result in tension of heart & blood vessel.
Clinical features :-
1. Lungs may collapse
2. Mediastinal shift
4.Hemothorax-
Accumulation of bloos in intrapleural space . it is mostly associated with open pneumothorax.
Causes:-
1. Cheast trauma
2. Lung malignancy
3. Comlication of anticoagulant therapy
4. Pulmonary embolism
5. Tearing of pleural adhesions
5.Cyclothorax:
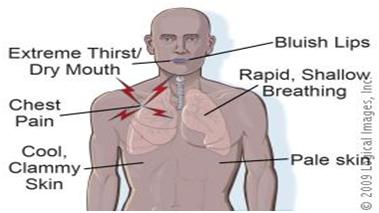
If pneumothorax is mild tachycardia &dyspnea will occur . if it is severe in condition respiratory distress, severe dyspnea, rapid breathing &air hunger which isa severe form of respiratory distress , chest pain , cough with or without haemoptysis , anxiety
DIAGNOSTIC EVALUATION:-
1. Physical examination on auscultation no breath sounds over the affected area
2. Cheast x rays shows the pressure & shadow of pneumothorax
3. Examination of purcussion shows hyper ressonance.
Medical management :-
1. It depends on cause or severity of the diseasecondition in mild cases constructive treatment ilke oxygen administration should be provided
2. In severe cases cheast drainage should be done small chest trube is inserted into the second intercostal space , in caes of severe accumulation the tube is inserted into 4th intercostal space to remove the accumulated air .
SURGICAL MANAGEMENT:-
1. In case of repeated pneumothorax pleuroctomy may be done
2. Pleurodysis:-
Artificial production of adhesions between visceral 7 parietal pleura with the help of chemical agent.
3. Needle venting :-
Pricking a large bore needle into the thorax to remove accumulated air
NURSING MANAGEMENT :-
1. PROVIDE SUPPLIMENT OXYGEN PLACE THE PATIENT IN SEMIFOWLERS POSITION.
2. OBTAIN TRAY FOR DRAIN OUT THE ACCUMULATED SUBSTANCES
3. AFTER DRAINAGE ASK THE PATIENT TO REPORT ANY INCREASE DYSPNEA
4. PALOPATED FOR SUBCUTENEOUS EMPHYSEMA IN UPPER CHEAST & NECK REGION.
Author: Tarun Mudgal