
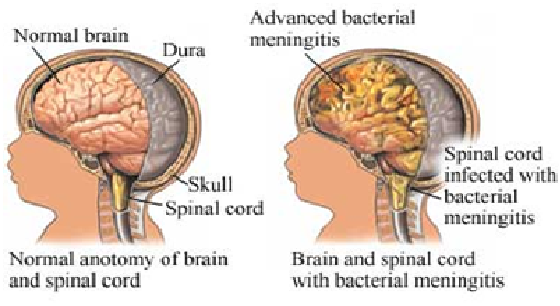
Meningitis is an inflammation of the linings around the brain and spinal cord caused by bacteria .
Causative agents:- Streptococcus pyogenes , niesseria meningitides and haemophilus influenza.
Risk factors:- -winter and early spring season.
-Viral upper respiratory infection.
-Otitis media.
-Immune system deficiency.
PATHOPHYSIOLOGY:- Once the causative agent enters the bloodstream,it crosses the blood brain barrier and proliferates in the cerebro spinal fluid. The host immune response stimulates the release of cell wall fragments and lipopolysaccharides ,facilitating of the subarachnoid and pia mater.
Because the cranial vault contains little room for expansion ,the inflammation may cause increased intracranial pressure. Crebro spinal fluid circulates through the subarachnoid space ,where inflammatory cellular materials from the affected meningeal tissue enter and accumulate,as a result clinical manifestation occurs.
CLINICAL MANIFESTATION:- Initial symptoms are headache and fever.
. Neck immobility.
. Positive kerning sign.
.Positive brudzinskis sign.
.Photophobia.
.Disorientation and memory impairement.
.Lethargy, unresponsiveness and coma.
.Seizures and increased intra cranial pressure.
.Brain stem herniation.
.Septicemia.
.Shock.
.Disseminated intravascular coagulation .
DIAGNOSTIC EVALUATION:- . Positive clinical manifestation.
. CT scan and MRI.
.Bacterial culture and gram staining .
.Glassgow coma scale.
MEDICAL MANAGEMENT:- . Vancomycin hydrochloride in combination with one of the cephalosporins is administered intravenously.
. Dexamethasone is administered 15 to 20 minutes before the first dose of antibiotic and every 6 hours for the next 4 days.
.Fluid volume expanders is given.
. Phenitoin is given to control the seizures.
NURSING MANAGEMENT:-
1. Neurological status and vital signs are assessed regularly.
2. Protecting the patient from injury secondary to seizures activity.
3. Preventing complications associated with immobility , such as pressure ulcers and pneumonia.
4. Instituting infection control precautions until 24 hours after initiation of antibiotic therapy.
5. Blood pressure is assessed for incipient shock ,which precedes cardiac or respiratory failure.
6. Insertion of a cuffed endotrachial tube and mechanical ventilation may be necessary to maintain adequate tissue ventilation.
7. Monitoring daily body weight ,serum electrolytes and urine volume ,specific gravity and osmolality ,especially if the syndrome of inappropriate anti diuretic hormone is suspected.
