
DESCRPITION
DEFINITION
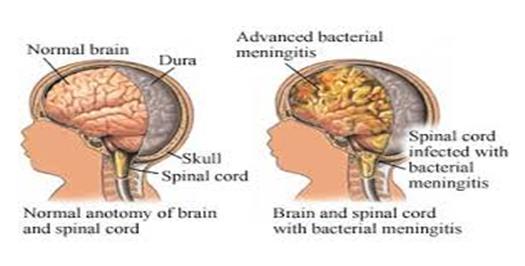
The inflammation of meninges (membranes surrounding the brain and spinal cord) which is caused by viral, bacterial or fungal organisms.
Classification
There are three classifications –
1. Aseptic – viral or causes or meningeal irritation from other causes such as brain abscess, encephalitis, leukaemia etc.
2. Septic — bacterial origin ex. Meningococcus, Neisseria meningitides, Staphylococcus, Influenza Bacillus.
3. Tuberculous – Tubercle Bacillus
Pathophysiology
The causative organisms enter the blood stream, cross the blood brain barrier, and trigger an inflammatory reaction in the meninges. Independent of the causative agents, inflammation of the subarachnoid and piamater occurs. Increased intra cranial pressure results. Meningeal infections generally originate in one of two ways: either through the blood stream from other infections or by direct extensions. In a few cases, the cause is iatrogenic or secondary to invasive procedures or devices.
Bacterial meningitis is the most significant form. The common bacterial pathogens are Neisseria meningitides, Streptococcus, Pneumoniae and Haemophylus Influenzae.
Clinical signs
Headache, Neck stiffness, Photophobia (intolerance to bright light), Irritability
Changes in level of consciousness, disorientation, memory impairment
Behavioural changes, coma
Positive Kernig’s sign
Vomiting bradycardia, increased ICP (intra cranial pressure)
Phonophobia (intolerance to loud noises)
Abnormal skin colour, cold extremities
Petechial rash
Morphology
• Grossly, pyogenic meningitis shows a thick layer of supportive exudates covers the leptomenings over the surface of the brain.
Diagnosis
• Culture of CSF
• Blood culture
• Urine specimen
• MRI
• CT-Scan
Management
1. Medical management
• Antimicrobial therapy- penicillin, ampicillin chloramphenicol
• Vancomycin, along with refampin is given for bacterial infection
• For dehydration or shock, fluid volume expenders are given
• Seizures are controlled by diazepam or phentoin
• Osmotic diuretics used to treat cerebral edema ex. Mannitol
2. Nursing management
• Management resolve around, prevention of dehydration, electrolytes imbalance and edema and fever.
• Body weight, serum electrolyte and urine volume are closely monitored.
• Arterial pressure is monitored to asses cardiac or respiratory failure and risk of shock
• Asses the patient neurologic status.
• Watch for cyanosis, cold extremities.
• Administer I.V. (intra venous) fluids and medications.
• Monitor vital signs and neurological status.
• Provide basic patients need care.
Complications
The complications of meningitis can be severe. The longer persistent in a human and child without treatment, the greater the risk of seizures permanent neurological damage including-
• Hearing loss
• Memory difficulty
• Learning disabilities
• Brain damage
• Gait problems
• Seizures
• Kidney failure
